
You are now leaving the site
Are you sure you want to leave?
Are you sure you want to leave?

1 given every 3 weeks1
*If not well tolerated, the minimum infusion duration should remain at 90 minutes.
The below charts are intended to provide dosing calculations for each infusion stage for patients ranging from 40 kg to 182 kg. The dosing values can also be downloaded as a PDF.
Determine the dosing and infusion values for your patient1
| Patient Weight | Infusion 1 (10 mg/kg) | Infusions 2 to 8 (20 mg/kg) | |||||
|---|---|---|---|---|---|---|---|
| lb* | kg* | Dose (mg) | Vials required (#) | Volume to withdraw (mL)† | Dose (mg) | Vials required (#) | Volume to withdraw (mL)† |
| 88 | 40 | 400 | 1 | 8.0 | 800 | 2 | 16.8 |
| 90 | 41 | 410 | 1 | 8.6 | 820 | 2 | 17.2 |
| 93 | 42 | 420 | 1 | 8.8 | 840 | 2 | 17.6 |
| 95 | 43 | 430 | 1 | 9.0 | 860 | 2 | 18.1 |
| 97 | 44 | 440 | 1 | 9.2 | 880 | 2 | 18.5 |
| 99 | 45 | 450 | 1 | 9.5 | 900 | 2 | 18.9 |
| 101 | 46 | 460 | 1 | 9.7 | 920 | 2 | 19.3 |
| 104 | 47 | 470 | 1 | 9.9 | 940 | 2 | 19.7 |
| 106 | 48 | 480 | 1 | 10.1 | 960 | 2 | 20.2 |
| 108 | 49 | 490 | 1 | 10.4 | 980 | 2 | 20.6 |
| 110 | 50 | 500 | 1 | 10.6 | 1000 | 2 | 21.0 |
| 112 | 51 | 510 | 2 | 10.7 | 1020 | 3 | 21.4 |
| 115 | 52 | 520 | 2 | 10.9 | 1040 | 3 | 21.8 |
| 117 | 53 | 530 | 2 | 11.1 | 1060 | 3 | 22.3 |
| 119 | 54 | 540 | 2 | 11.3 | 1080 | 3 | 22.7 |
| 121 | 55 | 550 | 2 | 11.6 | 1100 | 3 | 23.1 |
| 123 | 56 | 560 | 2 | 11.8 | 1120 | 3 | 23.5 |
| 126 | 57 | 570 | 2 | 12.0 | 1140 | 3 | 23.9 |
| 128 | 58 | 580 | 2 | 12.2 | 1160 | 3 | 24.4 |
| 130 | 59 | 590 | 2 | 12.4 | 1180 | 3 | 24.8 |
| 132 | 60 | 600 | 2 | 12.6 | 1200 | 3 | 25.2 |
| 135 | 61 | 610 | 2 | 12.9 | 1220 | 3 | 25.6 |
| 137 | 62 | 620 | 2 | 13.1 | 1240 | 3 | 26.1 |
| 139 | 63 | 630 | 2 | 13.2 | 1260 | 3 | 26.5 |
| 141 | 64 | 640 | 2 | 13.4 | 1280 | 3 | 26.9 |
| 143 | 65 | 650 | 2 | 13.7 | 1300 | 3 | 27.3 |
| 146 | 66 | 660 | 2 | 13.9 | 1320 | 3 | 27.7 |
| 148 | 67 | 670 | 2 | 14.1 | 1340 | 3 | 28.1 |
| 150 | 68 | 680 | 2 | 14.3 | 1360 | 3 | 28.6 |
| 152 | 69 | 690 | 2 | 14.5 | 1380 | 3 | 29.0 |
| 154 | 70 | 700 | 2 | 14.7 | 1400 | 3 | 29.4 |
| 157 | 71 | 710 | 2 | 14.9 | 1420 | 3 | 29.8 |
| 159 | 72 | 720 | 2 | 15.2 | 1440 | 3 | 30.2 |
| 161 | 73 | 730 | 2 | 15.3 | 1460 | 3 | 30.7 |
| 163 | 74 | 740 | 2 | 15.5 | 1480 | 3 | 31.1 |
| 165 | 75 | 750 | 2 | 15.7 | 1500 | 3 | 31.5 |
| 168 | 76 | 760 | 2 | 15.9 | 1520 | 3 | 31.9 |
| Patient Weight | Infusion 1 (10 mg/kg) | Infusions 2 to 8 (20 mg/kg) | |||||
|---|---|---|---|---|---|---|---|
| lb* | kg* | Dose (mg) | Vials required(#) | Volume to withdraw (mL)† | Dose (mg) | Vials required(#) | Volume to withdraw (mL)† |
| 170 | 77 | 770 | 2 | 16.2 | 1540 | 4 | 32.4 |
| 172 | 78 | 780 | 2 | 16.4 | 1560 | 4 | 32.8 |
| 174 | 79 | 790 | 2 | 16.6 | 1580 | 4 | 33.2 |
| 176 | 80 | 800 | 2 | 16.8 | 1600 | 4 | 33.6 |
| 179 | 81 | 810 | 2 | 17.0 | 1620 | 4 | 34.0 |
| 181 | 82 | 820 | 2 | 17.2 | 1640 | 4 | 34.5 |
| 183 | 83 | 830 | 2 | 17.4 | 1660 | 4 | 34.9 |
| 185 | 84 | 840 | 2 | 17.6 | 1680 | 4 | 35.3 |
| 187 | 85 | 850 | 2 | 17.9 | 1700 | 4 | 35.7 |
| 190 | 86 | 860 | 2 | 18.1 | 1720 | 4 | 36.1 |
| 192 | 87 | 870 | 2 | 18.3 | 1740 | 4 | 36.6 |
| 194 | 88 | 880 | 2 | 18.5 | 1760 | 4 | 37.0 |
| 196 | 89 | 890 | 2 | 18.7 | 1780 | 4 | 37.4 |
| 198 | 90 | 900 | 2 | 18.9 | 1800 | 4 | 37.8 |
| 201 | 91 | 910 | 2 | 19.1 | 1820 | 4 | 38.2 |
| 203 | 92 | 920 | 2 | 19.3 | 1840 | 4 | 38.7 |
| 205 | 93 | 930 | 2 | 19.5 | 1860 | 4 | 39.1 |
| 207 | 94 | 940 | 2 | 19.7 | 1880 | 4 | 39.5 |
| 209 | 95 | 950 | 2 | 20.0 | 1900 | 4 | 39.9 |
| 212 | 96 | 960 | 2 | 20.2 | 1920 | 4 | 40.3 |
| 214 | 97 | 970 | 2 | 20.4 | 1940 | 4 | 40.8 |
| 216 | 98 | 980 | 2 | 20.6 | 1960 | 4 | 41.2 |
| 218 | 99 | 990 | 2 | 20.8 | 1980 | 4 | 41.6 |
| 221 | 100 | 1000 | 2 | 21.0 | 2000 | 4 | 42.0 |
| 223 | 101 | 1010 | 3 | 21.2 | 2020 | 5 | 42.4 |
| 225 | 102 | 1020 | 3 | 21.4 | 2040 | 5 | 42.9 |
| 227 | 103 | 1030 | 3 | 21.6 | 2060 | 5 | 43.3 |
| 229 | 104 | 1040 | 3 | 21.8 | 2080 | 5 | 43.7 |
| 232 | 105 | 1050 | 3 | 22.1 | 2100 | 5 | 44.1 |
| 234 | 106 | 1060 | 3 | 22.3 | 2120 | 5 | 44.5 |
| 236 | 107 | 1070 | 3 | 22.5 | 2140 | 5 | 45.0 |
| 238 | 108 | 1080 | 3 | 22.7 | 2160 | 5 | 45.4 |
| 240 | 109 | 1090 | 3 | 22.9 | 2180 | 5 | 45.8 |
| 243 | 110 | 1100 | 3 | 23.1 | 2200 | 5 | 46.2 |
| 245 | 111 | 1110 | 3 | 23.3 | 2220 | 5 | 46.6 |
| 247 | 112 | 1120 | 3 | 23.5 | 2240 | 5 | 47.1 |
| Patient Weight | Infusion 1 (10 mg/kg) | Infusions 2 to 8 (20 mg/kg) | |||||
|---|---|---|---|---|---|---|---|
| lb* | kg* | Dose (mg) | Vials required (#) | Volume to withdraw (mL)† | Dose (mg) | Vials required (#) | Volume to withdraw (mL)† |
| 249 | 113 | 1130 | 3 | 23.7 | 2260 | 5 | 47.5 |
| 251 | 114 | 1140 | 3 | 23.9 | 2280 | 5 | 47.9 |
| 254 | 115 | 1150 | 3 | 24.2 | 2300 | 5 | 48.3 |
| 256 | 116 | 1160 | 3 | 24.4 | 2320 | 5 | 48.7 |
| 258 | 117 | 1170 | 3 | 24.6 | 2340 | 5 | 49.2 |
| 260 | 118 | 1180 | 3 | 24.8 | 2360 | 5 | 49.6 |
| 262 | 119 | 1190 | 3 | 25.0 | 2380 | 5 | 50.0 |
| 265 | 120 | 1200 | 3 | 25.2 | 2400 | 5 | 50.4 |
| 267 | 121 | 1210 | 3 | 25.4 | 2420 | 5 | 50.8 |
| 269 | 122 | 1220 | 3 | 25.6 | 2440 | 5 | 51.3 |
| 271 | 123 | 1230 | 3 | 25.8 | 2460 | 5 | 51.7 |
| 273 | 124 | 1240 | 3 | 26.1 | 2480 | 5 | 52.1 |
| 276 | 125 | 1250 | 3 | 26.3 | 2500 | 5 | 52.5 |
| 278 | 126 | 1260 | 3 | 26.5 | 2520 | 6 | 52.9 |
| 280 | 127 | 1270 | 3 | 26.7 | 2540 | 6 | 53.4 |
| 282 | 128 | 1280 | 3 | 26.9 | 2560 | 6 | 53.8 |
| 284 | 129 | 1290 | 3 | 27.1 | 2580 | 6 | 54.2 |
| 287 | 130 | 1300 | 3 | 27.3 | 2600 | 6 | 54.6 |
| 289 | 131 | 1310 | 3 | 27.5 | 2620 | 6 | 55.0 |
| 291 | 132 | 1320 | 3 | 27.7 | 2640 | 6 | 55.5 |
| 293 | 133 | 1330 | 3 | 27.9 | 2660 | 6 | 55.9 |
| 295 | 134 | 1340 | 3 | 28.2 | 2680 | 6 | 56.3 |
| 298 | 135 | 1350 | 3 | 28.4 | 2700 | 6 | 56.7 |
| 300 | 136 | 1360 | 3 | 28.6 | 2720 | 6 | 57.1 |
| 302 | 137 | 1370 | 3 | 28.8 | 2740 | 6 | 57.6 |
| 304 | 138 | 1380 | 3 | 29.0 | 2760 | 6 | 58.0 |
| 306 | 139 | 1390 | 3 | 29.2 | 2780 | 6 | 58.4 |
| 309 | 140 | 1400 | 3 | 29.4 | 2800 | 6 | 58.8 |
| 311 | 141 | 1410 | 3 | 29.6 | 2820 | 6 | 59.2 |
| 313 | 142 | 1420 | 3 | 29.8 | 2840 | 6 | 59.7 |
| 315 | 143 | 1430 | 3 | 30.0 | 2860 | 6 | 60.1 |
| 318 | 144 | 1440 | 3 | 30.3 | 2880 | 6 | 60.5 |
| 320 | 145 | 1450 | 3 | 30.5 | 2900 | 6 | 60.9 |
| 322 | 146 | 1460 | 3 | 30.7 | 2920 | 6 | 61.3 |
| 324 | 147 | 1470 | 3 | 30.9 | 2940 | 6 | 61.8 |
| 326 | 148 | 1480 | 3 | 31.1 | 2960 | 6 | 62.2 |
| Patient Weight | Infusion 1 (1.0 mg/kg) | Infusions 2 to 8 (20 mg/kg) | |||||
|---|---|---|---|---|---|---|---|
| lb* | kg* | Dose (mg) | Vials required(#) | Volume to withdraw (mL)† | Dose (mg) | Vials required(#) | Volume to withdraw (mL)† |
| 329 | 145 | 1490 | 3 | 31.1 | 2960 | 6 | 62.6 |
| 331 | 150 | 1500 | 3 | 31.5 | 3000 | 6 | 63.0 |
| 333 | 151 | 1510 | 4 | 31.7 | 3020 | 7 | 63.4 |
| 335 | 152 | 1520 | 4 | 31.9 | 3040 | 7 | 63.9 |
| 337 | 153 | 1530 | 4 | 32.1 | 3060 | 7 | 64.3 |
| 340 | 154 | 1540 | 4 | 32.4 | 3080 | 7 | 64.7 |
| 342 | 155 | 1550 | 4 | 32.6 | 3100 | 7 | 65.1 |
| 344 | 156 | 1560 | 4 | 32.8 | 3120 | 7 | 65.5 |
| 346 | 157 | 1570 | 4 | 33.0 | 3140 | 7 | 66.0 |
| 348 | 158 | 1580 | 4 | 33.2 | 3160 | 7 | 66.4 |
| 351 | 159 | 1590 | 4 | 33.4 | 3180 | 7 | 66.8 |
| 353 | 160 | 1600 | 4 | 33.6 | 3200 | 7 | 67.2 |
| 355 | 161 | 1610 | 4 | 33.8 | 3220 | 7 | 67.6 |
| 357 | 162 | 1620 | 4 | 34.0 | 3240 | 7 | 68.1 |
| 359 | 163 | 1630 | 4 | 34.2 | 3260 | 7 | 68.5 |
| 362 | 164 | 1640 | 4 | 34.5 | 3280 | 7 | 68.9 |
| 364 | 165 | 1650 | 4 | 34.7 | 3300 | 7 | 69.3 |
| 366 | 166 | 1660 | 4 | 34.9 | 3320 | 7 | 69.7 |
| 368 | 167 | 1670 | 4 | 35.1 | 3340 | 7 | 70.2 |
| 370 | 168 | 1680 | 4 | 35.3 | 3360 | 7 | 70.6 |
| 373 | 169 | 1690 | 4 | 35.5 | 3380 | 7 | 71.0 |
| 375 | 170 | 1700 | 4 | 35.7 | 3400 | 7 | 71.4 |
| 377 | 171 | 1710 | 4 | 35.9 | 3420 | 7 | 71.8 |
| 379 | 172 | 1720 | 4 | 36.1 | 3440 | 7 | 72.3 |
| 381 | 173 | 1730 | 4 | 36.3 | 3460 | 7 | 72.7 |
| 384 | 174 | 1740 | 4 | 36.6 | 3480 | 7 | 73.1 |
| 386 | 175 | 1750 | 4 | 36.8 | 3500 | 7 | 73.5 |
| 388 | 176 | 1760 | 4 | 37.0 | 3520 | 8 | 73.9 |
| 390 | 177 | 1770 | 4 | 37.2 | 3540 | 8 | 74.4 |
| 392 | 178 | 1780 | 4 | 37.4 | 3560 | 8 | 74.8 |
| 395 | 179 | 1790 | 4 | 37.6 | 3580 | 8 | 75.2 |
| 397 | 180 | 1800 | 4 | 37.8 | 3600 | 8 | 75.6 |
| 399 | 181 | 1810 | 4 | 38.0 | 3620 | 8 | 76.1 |
| 401 | 182 | 1820 | 4 | 38.2 | 3640 | 8 | 76.5 |
*Rounded to the nearest whole number.
†Rounded to the nearest tenth.

If dose is <1800 mg, use a 100-mL bag of normal saline (0.9% NaCl)1
If dose is ≥1800 mg, use a 250-mL bag of normal saline (0.9% NaCl)1
IV, intravenous.
All TEPEZZA patients completing treatment had proptosis reduction3,*
Phase 3 study exploratory analysis: Change from baseline in proptosis over 24 weeks in individual patients
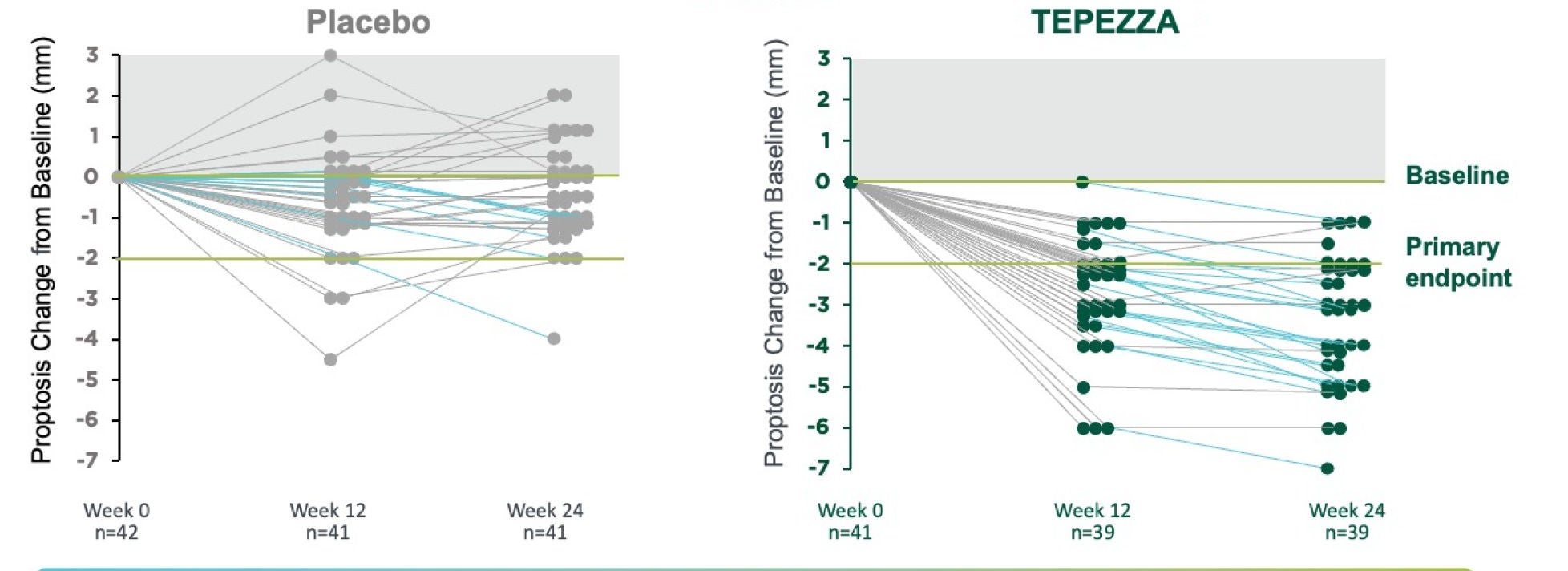


In a post hoc analysis, 63% (n=15/24) of TEPEZZA patients who showed no proptosis improvement midway (12 weeks) through treatment ultimately did have a proptosis response after completing 8 infusions at 24 weeks from baseline.2
*Analysis is exploratory and has not been adjusted for multiple comparisons. No conclusions of statistical or clinical significance can be drawn.

"After the second infusion, my symptoms seemed to decrease, and that motivated me to continue."
—Randi C., real TEPEZZA patient
In the Phase 3 study, improvement of proptosis as measured by mean change from baseline was observed as early as 6 weeks and continued to improve through Week 24.1


patients with TED would prefer IV medicine before trying eye surgery4
Based on a survey of 102 TED patients.
Receive the latest news and updates about TEPEZZA
Receive the latest news and updates about TEPEZZA
WARNINGS AND PRECAUTIONS
Infusion Reactions: TEPEZZA may cause infusion reactions. Infusion reactions have been reported in approximately 4% of patients treated with TEPEZZA. Reported infusion reactions have usually been mild or moderate in severity. Signs and symptoms may include transient increases in blood pressure, feeling hot, tachycardia, dyspnea, headache, and muscular pain. Infusion reactions may occur during an infusion or within 1.5 hours after an infusion. In patients who experience an infusion reaction, consideration should be given to premedicating with an antihistamine, antipyretic, or corticosteroid and/or administering all subsequent infusions at a slower infusion rate.
Inflammatory Bowel Disease: TEPEZZA may cause an exacerbation of inflammatory bowel disease (IBD). IBD has been reported in some patients without a prior diagnosis of IBD. Monitor patients for signs and symptoms of IBD. If IBD exacerbation is suspected, discontinue use of TEPEZZA.
Hyperglycemia: Increased blood glucose or hyperglycemia may occur in patients treated with TEPEZZA. In clinical trials, 10% of patients (two-thirds of whom had preexisting diabetes or impaired glucose tolerance) experienced hyperglycemia. Hyperglycemic events should be controlled with medications for glycemic control, if necessary. Assess patients for elevated blood glucose and symptoms of hyperglycemia prior to infusion and continue to monitor while on treatment with TEPEZZA. Ensure patients with hyperglycemia or preexisting diabetes are under appropriate glycemic control before and while receiving TEPEZZA.
Hearing Impairment Including Hearing Loss: TEPEZZA may cause severe hearing impairment including hearing loss, which in some cases may be permanent. Assess patients’ hearing before, during, and after treatment with TEPEZZA and consider the benefit-risk of treatment with patients.
ADVERSE REACTIONS
The most common adverse reactions (incidence ≥5% and greater than placebo) are muscle spasm, nausea, alopecia, diarrhea, fatigue, hyperglycemia, hearing impairment, dysgeusia, headache, dry skin, ear discomfort, weight decreased, nail disorders, and menstrual disorders.
INDICATION
TEPEZZA is indicated for the treatment of Thyroid Eye Disease regardless of Thyroid Eye Disease activity or duration.
Please see Full Prescribing Information for more information.
1. TEPEZZA (teprotumumab-trbw) [prescribing information] Amgen. 2. Ugradar S, Wang Y, Mester T, et al. Teprotumumab for thyroid eye disease: early response is not required for benefit. Eye (Lond). 2022;36(7):1403-1408. 3. Supplement to: Douglas RS, Kahaly GJ, Patel A, et al. Teprotumumab for the treatment of active thyroid eye disease. N Engl J Med. 2020;382(4):341-352. 4. Data on File. Amgen, January 2023.

