
You are now leaving the site
Are you sure you want to leave?
Are you sure you want to leave?
Receive the latest news and updates about TEPEZZA
Receive the latest news and updates about TEPEZZA

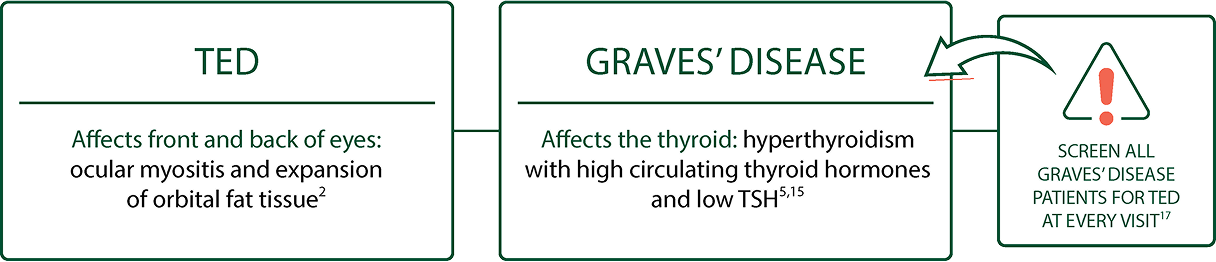
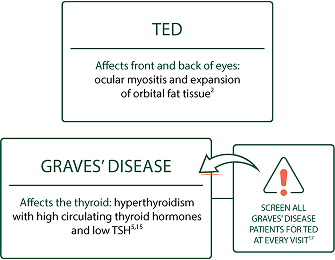
Treating only the thyroid won’t treat TED2-5
Even TED patients who have had their thyroid gland completely removed can continue to suffer6-8
IGF-1R activation on orbital fibroblasts leads to inflammation and expansion of muscle and fat tissue behind the eye2-4,9

In a study of patients with untreated Graves’ disease and no diagnosed clinical ophthalmopathy, 71% (n=17) showed extraocular muscle swelling in orbital MRI11

Like other autoimmune diseases, patients with TED experience disease flares13,14
In a retrospective chart review of 415 patients, 16% (65) were identified as having disease flares/recurrent TED, regardless of initial treatment1,*
*Recurrent TED was evidenced by prior medical or surgical intervention for TED, prior orbital imaging with diagnostic evidence for TED, or patient report of painless orbital inflammatory disease or photographs demonstrating a change in appearance consistent with TED.1
IGF-1R, insulin-like growth factor-1 receptor; MRI, magnetic resonance imaging; TED, Thyroid Eye Disease.


Images provided with permission from Jody Abrams, MD.
Images provided with permission from Mark Lupo, MD.
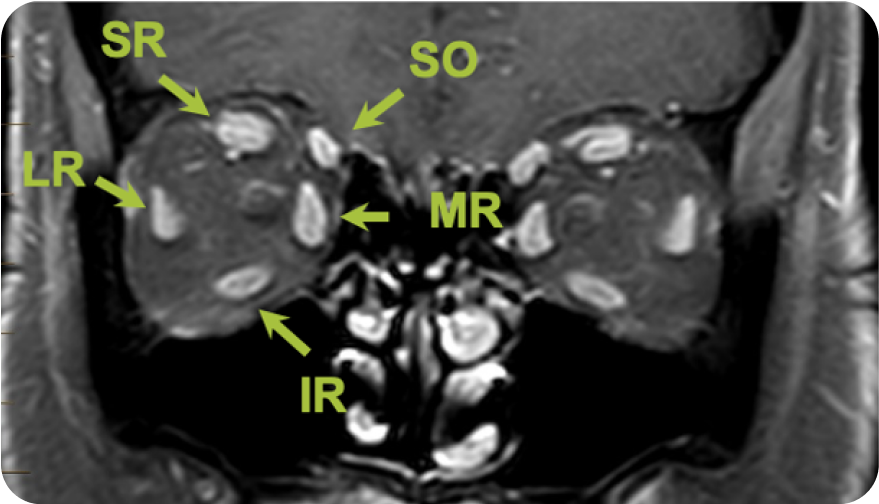
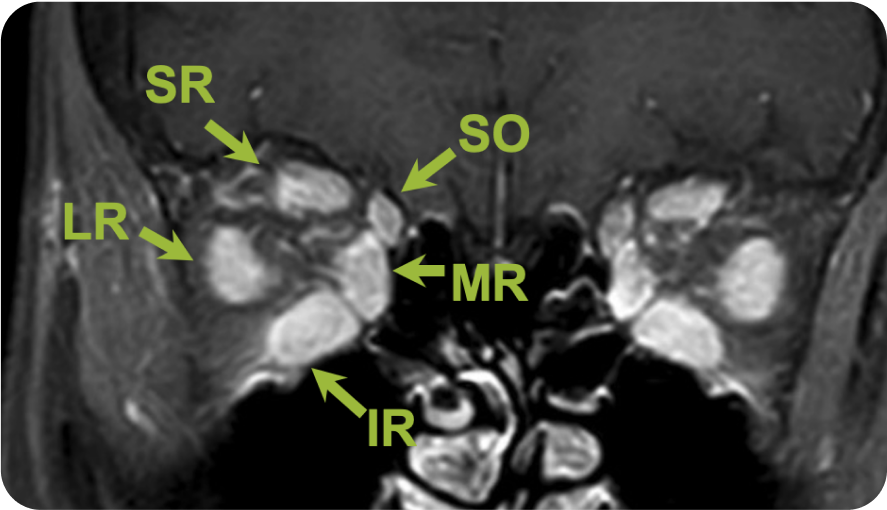
IR, inferior rectus; LR, lateral rectus; MR, medial rectus; SO, superior oblique; SR, superior rectus.
Green arrows point to a coronal view of the extraocular muscles (white areas)
Extraocular muscle volume increase in patients with TED
TED is more than proptosis. If your patients with thyroid conditions present with any of the following signs or symptoms, it could be TED9
Proptosis
Eyelid retraction
Redness, swelling, and excessive tearing
Soft tissue changes around eyes
Diplopia
Blurry vision
Itchy eyes
Dryness and grittiness
Pressure/Pain behind the eye
Photophobia
Color vision loss⁹
TSH, thyroid-stimulating hormone.

Patients with TED often show symptoms of dry eye disease19
DRY EYE DISEASE (DED): Affects lacrimal glands and ocular surface causing insufficient lubrication to aqueous tear-film layer20
The visible and nonvisible symptoms of TED can have a debilitating impact on your patients’ daily activities and self-confidence21-23

(n=242/394)

(n=177/394)
Based on an online 62-question survey of 443 TED patients with a diagnosis that ranged from <1 to >10 years23


(n=50/70)
Based on responses from 70 patients with TED with a duration of disease ranging from 12 to 18 months who answered 16 questions from the GO-QOL questionnaire24
GO-QOL, Graves’ Ophthalmopathy Quality of Life.

— Kim E, Patient with TED
Consider the signs and symptoms of TED, as well as patients’ ability to manage daily activities, for a deeper understanding of disease burden
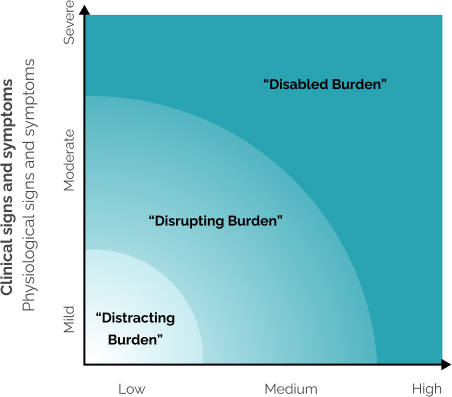
Patient-Reported Impact
Degree to which symptoms impact patients’ daily
activities and emotional well-being
Not an official medical tool.
The Patient Intake Form includes the Burden-Impact Model—ask your AMGEN representative for a copy.


Some examples: walking outdoors, driving, reading


Some examples: negative impact to self-esteem, hiding their appearance in public


I’m Kim, and this is my journey with Thyroid Eye Disease. When I was 17, I started to get really tired, and my mom was worried about me, so she took me to the doctor to have me checked for Mono. And the doctor did the blood work and said, you do not have Mono. I think it’s just growing pains and kind of just sent me on my way.
And then I went to college where I was recruited to play volleyball and run track. When I went to the volleyball camp before the season, the coach called me into the office and she looked at me and she said, “You play like you’re sick, I’m cutting you.” And I was devastated. So, I went to a doctor on campus and he basically told me I was a hypochondriac.
My uncle is an ophthalmologist and he looked at me and said, ” Oh my gosh, you are so sick.” My uncle got me into an endocrinologist, and he said, “You have Graves’ disease, and you need treatments immediately.”
So, I started radiation treatments. Once that was stabilized, my eye symptoms started to get worse. And my uncle at that time said, “You have Thyroid Eye Disease and it is independent from your Grave’s disease.” I had the tightness in my eyes. The bulging. And they kept getting worse and worse as time was going on. My eyelids wouldn’t close. So, they got me into an ocular plastic surgeon and I had my first Levator surgery. That took care of the major symptoms.
I could drive during the day, but nighttime no, everything, all the lights were double. You just kind of learn to live with those symptoms and move on because you think there’s nothing you can do anymore. So, I thought this is just how it was going to be. You just aren’t comfortable anymore with yourself in your own skin and everything bothers you.
It got to a point where I didn’t want to be out in public because people would look at me and I knew they were looking at my eyes.
After 25 years and four surgeries, my optometrist recommended that I see an oculoplastic surgeon, and the new oculoplastic surgeon said, “Hey, there’s this new medicine out called TEPEZZA. I think before we do any more surgeries on you, you should try it.” I had told her I saw the commercials, and I said I didn’t think it was an option for me because I thought I had to be in that bad phase with all those bad symptoms I had before. And she said, “No, I’m pretty sure this is going to be it.”
When I went for my first infusion, I was very anxious. Then after the second treatment, I got used to everything. And then after the fourth treatment, I noticed the bulging had decreased. It was exciting to, to see that. The most significant difference was infusions five through eight. The tightness was gone. When I was done, my eye bulging, decreased three millimeters in each eye, which is a significant difference.
To see myself now, after this treatment, it’s been uplifting because I don’t think about my eyes every day anymore. I can go about my day being confident and people aren’t asking me about my eyes. When my son got married, I actually couldn’t wait to see the pictures. And you see a picture. You don’t see eyes. It’s been an amazing experience. If I can help somebody who was in the same stage as I was and thinks they can’t do this, they should make sure they ask their doctor, “is this an option for me?” Because I didn’t think it was and it’s been incredible.
Talk to your doctor to see if TEPEZZA might be right for you.
WARNINGS AND PRECAUTIONS
Infusion Reactions: TEPEZZA may cause infusion reactions. Infusion reactions have been reported in approximately 4% of patients treated with TEPEZZA. Reported infusion reactions have usually been mild or moderate in severity. Signs and symptoms may include transient increases in blood pressure, feeling hot, tachycardia, dyspnea, headache, and muscular pain. Infusion reactions may occur during an infusion or within 1.5 hours after an infusion. In patients who experience an infusion reaction, consideration should be given to premedicating with an antihistamine, antipyretic, or corticosteroid and/or administering all subsequent infusions at a slower infusion rate.
Inflammatory Bowel Disease: TEPEZZA may cause an exacerbation of inflammatory bowel disease (IBD). IBD has been reported in some patients without a prior diagnosis of IBD. Monitor patients for signs and symptoms of IBD. If IBD exacerbation is suspected, discontinue use of TEPEZZA.
Hyperglycemia: Increased blood glucose or hyperglycemia may occur in patients treated with TEPEZZA. In clinical trials, 10% of patients (two-thirds of whom had preexisting diabetes or impaired glucose tolerance) experienced hyperglycemia. Hyperglycemic events should be controlled with medications for glycemic control, if necessary. Assess patients for elevated blood glucose and symptoms of hyperglycemia prior to infusion and continue to monitor while on treatment with TEPEZZA. Ensure patients with hyperglycemia or preexisting diabetes are under appropriate glycemic control before and while receiving TEPEZZA.
Hearing Impairment Including Hearing Loss: TEPEZZA may cause severe hearing impairment including hearing loss, which in some cases may be permanent. Assess patients’ hearing before, during, and after treatment with TEPEZZA and consider the benefit-risk of treatment with patients.
ADVERSE REACTIONS
The most common adverse reactions (incidence ≥5% and greater than placebo) are muscle spasm, nausea, alopecia, diarrhea, fatigue, hyperglycemia, hearing impairment, dysgeusia, headache, dry skin, ear discomfort, weight decreased, nail disorders, and menstrual disorders.
INDICATION
TEPEZZA is indicated for the treatment of Thyroid Eye Disease regardless of Thyroid Eye Disease activity or duration.
Please see Full Prescribing Information for more information.
1. Patel P, Khandji J, Kazim M. Recurrent Thyroid Eye Disease. Ophthalmic Plast Reconstr Surg. 2015;31(6):445-448. 2. Patel A, Yang H, Douglas RS. A new era in the treatment of thyroid eye disease. Am J Ophthalmol. 2019;208:281-288. 3. Bahn RS. Graves' ophthalmopathy. N Engl J Med. 2010;362(8):726-738. 4. Wang Y, Patel A, Douglas RS. Thyroid Eye Disease: how a novel therapy may change the treatment paradigm. Ther Clin Risk Manag. 2019:15:1305-1318. 5. Smith TJ, Hegedüs L. Graves' disease. N Engl J Med. 2016;375(16):1552-1665. 6. Bartley GB. The epidemiologic characteristics and clinical course of ophthalmopathy associated with autoimmune thyroid disease in Olmsted County. Minnesota. Trans Am Ophthalmol Soc. 1994;92:477-588. 7. Gwinup G, Elias AN, Ascher MS. Effect on exophthalmos of various methods of treatment of Graves' disease. JAMA. 1982;247(15):2135-2138. 8. Tallstedt L, Lundell G, Torring O, Wallin G. Ljunggren JG, Blomgren H, Taube A. Occurrence of ophthalmopathy after treatment for Graves' hyperthyroidism. The Thyroid Study Group. N Engl J Med. 1992;326(26):1733-1738. 9. Cockerham KP, Padnick-Silver L, Stuertz N, Francis-Sedlak L. Holt RJ. Quality of life in patients with chronic Thyroid Eye Disease in the United States. Ophthalmol Ther. 2021;10:975-987. 10. Kilicarslan R, Alkan A, Ilhan MM, et al. Graves' ophthalmopathy: the role of diffusion-weighted imaging in detecting involvement of extraocular muscles in early period of disease. Br J Radiol. 2015;88(1047):20140677. 11. Villadolid MC, Yokoyama N, Isumi M, et al. Untreated Graves' disease patients without clinical ophthalmopathy demonstrate a high frequency of extraocular muscle (EOM) enlargement by magnetic resonance. J Clin Endocrinol Metab. 1995;80(9):2830-2833. 12. Mahmoud QJ. Thyroid-associated orbitopathy: Radiology case. Radiopaedia. 2023. https://radiopaedia.org/cases/thyroid-associated-orbitopathy-23?lang=us. Accessed March 25, 2025. 13. Bartalena L, Krassas GE, Wiersinga W, et al. Efficacy and safety of three different cumulative doses of intravenous methylprednisolone for moderate to severe and active Graves' orbitopathy. J Clin Endocrinol Metab. 2012;97(12):4454-4463. 14. Hahn E, Laperriere N, Millar BA, et al. Orbital radiation therapy for Graves' ophthalmopathy: measuring clinical efficacy and impact. Pract Radiat Oncol. 2014;4(4):233-239. 15. Barrio-Barrio J, Sabater AL, Bonet-Farriol E. Velázquez-Villoria Á, Galofré JC. Graves' ophthalmopathy: VISA versus EUGOGO classification, assessment, and management. J Ophthalmol. 2015:2015:249125. 16. Bothun ED, Scheurer RA, Harrison AR, Lee MS. Update on thyroid eye disease and management. Clin Ophthalmol. 2009;3:543-551. 17. Burch HB, Perros P, Bednarczuk T, et al. Management of thyroid eye disease: a consensus statement by the American Thyroid Association and the European Thyroid Association. Thyroid. 2022;32(12):1-32. 18. Couch SM. Thyroid eye disease: timely diagnosis is the key to controlling this autoimmune condition. Glaucoma Today. January/February 2019. Accessed March 25, 2025. 19. Selter JH, Gire AI, Sikder S. The relationship between Graves' ophthalmopathy and dry eye syndrome. Clin Ophthalmol. 2015:9;57-62. 20. Verjee MA, Brissette AR, Starr CE. Dry eye disease: early recognition with guidance on management and treatment for primary care family physicians. Ophthalmol Ther. 2020;9:877-888. 21. Kahaly GJ, Petrak F, Hardt J, Pitz S, Egle UT. Psychosocial morbidity of Graves' orbitopathy. Clin Endocrinol (Oxf). 2005:63(4):395-402. 22. Estcourt S, Vaidya B, Quinn A, Shepherd M. The impact of thyroid eye disease upon patients' wellbeing: a qualitative analysis. Clin Endocrinol (Oxf). 2008:68(4):635-639. 23. Smith TJ, Cockerham K, Conrad E, Holt RJ. (2023, May 4-6). Assessment of the thyroid eye diseasespecific graves' ophthalmopathy quality of life questionnaire in non-inflammatory or inactive thyroid eye disease patients. American Association of Clinical Endocrinology meeting. Seattle WA. 24. Terwee CB, Gerding MN, Dekker FW, et al. Development of a disease specific quality of life questionnaire for patients with Graves’ ophthalmopathy: the GO-QOL. Br J Ophthalmol. 1998;82:773-779. 25. Park JJ, Sullivan TJ, Mortimer RH, et al. Assessing quality of life in Australian patients with Graves’ ophthalmopathy. Br J Ophthalmol. 2004 Jan;88(1):75-78.

